กรณีศึกษานี้ นำเสนอโดย นพ.พีระคง หล้าพันธ์ โรงพยาบาลราชวิถี
คลิ๊กที่ Tab ด้านล่างไปติดตามกันได้เลย
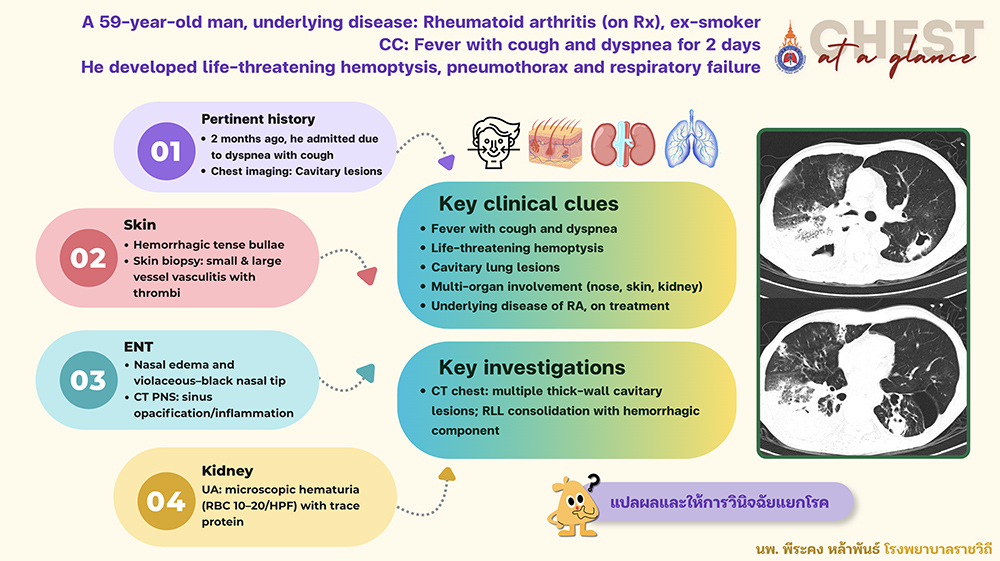
A 59-year-old man, ex-smoker
Underlying disease: Rheumatoid arthritis (on immunosuppressive drugs)
CC: Fever with cough and dyspnea for 2 days
He developed life-threatening hemoptysis, pneumothorax and respiratory failure
Pertinent history:
- 2 months ago, he admitted due to dyspnea with cough
- Chest imaging: cavitary lung lesions
Skin:
- Hemorrhagic tense bullae
- Skin biopsy: small and large vessel vasculitis with thrombi
ENT:
- Nasal edema and violaceous–black nasal tip
- CT PNS: paranasal sinus opacification and inflammation
Kidney:
UA: microscopic hematuria (RBC 10–20/HPF) with trace protein
สรุป key clinical clues
- Fever with cough and dyspnea
- Life-threatening hemoptysis
- Cavitary lung lesions
- Multi-organ involvement (nose, skin, kidney)
- Underlying disease of RA, on immunosuppressive drugs
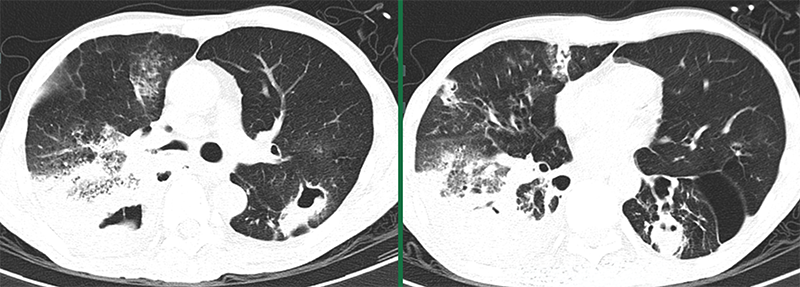
Chest CT
Multiple thick-wall cavitary lesions; RLL consolidation with hemorrhagic component
ลองแปลผลและให้การวินิจฉัยแยกโรคกันครับ แล้วคลิ๊กไปดูเฉลยกันที่ Tab ด้านบนต่อไปได้เลย
(ต่อ)
Differential diagnosis
- Lung abscess/necrotizing pneumonia (bacteria, TB, fungi)
- Granulomatous with polyangiitis (GPA)
- Solid malignancy
Further investigation
- BAL fluid culture: Corynebacterium striatum
- Transbronchial lung biopsy: negative for malignancy and granuloma
- ANCA testing: PR3/c-ANCA > 200 RU/mL และ MPO/p-ANCA <2 RU/mL
Definite diagnosis
Probable GPA (PR3-ANCA associated vasculitis) withsecondary spontaneous pneumothorax with persistent air leak
Treatment and progression
- Antibiotics: Vancomycin plus prior broad-spectrum antibiotics.
- Systemic therapy escalated for vasculitis: Dexamethasone → IV methylprednisolone → Rituximab
- Persistent air leak required multiple ICD revisions, pleurodesis, and endobronchial spigot insertion → full lung expansion and ICD removal.