นำเสนอโดย พญ. นลินพร ดีชาติ คณะแพทยศาสตร์วชิรพยาบาล มหาวิทยาลัยนวมินทราธิราช

A 62-year-old woman, no known underlying disease
CC: Dry cough for 6 months
Key clinical findings
- Persistent dry cough for 6 months
- Constitutional symptoms without fever
- Physical exam: coarse crepitation at left upper lung zone
Key investigations
- Hb 11.9 g/dL, Hct 38%, WBC 6,910 /uL (N 40%, L 33%, E 20%), platelet 280,000 cell/uL
- CXR : well-defined mass-like consolidation with reticulonodular infiltrates at left middle lung zone

ลองแปลผลและให้การวินิจฉัยแยกโรคกันครับ
Differential diagnosis จากประวัติ ตรวจร่างกาย และภาพ Chest X-ray
- Primary lung cancer
- Pulmonary lymphoma
- Chronic eosinophilic pneumonia แต่ไม่อธิบาย mass-liked lesion
- Allergic bronchopulmonary aspergillosis (ABPA) แต่ไม่มีอาการหอบเหนื่อยหรือประวัติคล้ายโรคหืดมาก่อน
Chest CT findings:
- Multifocal consolidation at lingula
- Dilated bronchus with high-attenuation mucus (H) (HAM) at lingula
การประเมิน mass-liked lesion ใน CT อาจต้องดูหลาย view ทั้ง axial view, coronal และ sagittal view (ไม่ได้แสดงในรูป) กรณีนี้ขอบชัดและเป็น tubular-shaped ต่อกับ bronchus จึงทำให้นึกถึงรอยโรคที่เป็น bronchiectasis มากกว่า lung mass
Chest CT เข้าได้กับ ABPA จึงส่งตรวจเพิ่มเติมดังนี้
- BAL fluid cultures: no growth all
- TBLB: chronic inflammation
- Total IgE >5,000 kU/L ↑
- Aspergillus fumigatus IgE 8.81 kU/L ↑
- Spirometry: mild obstruction
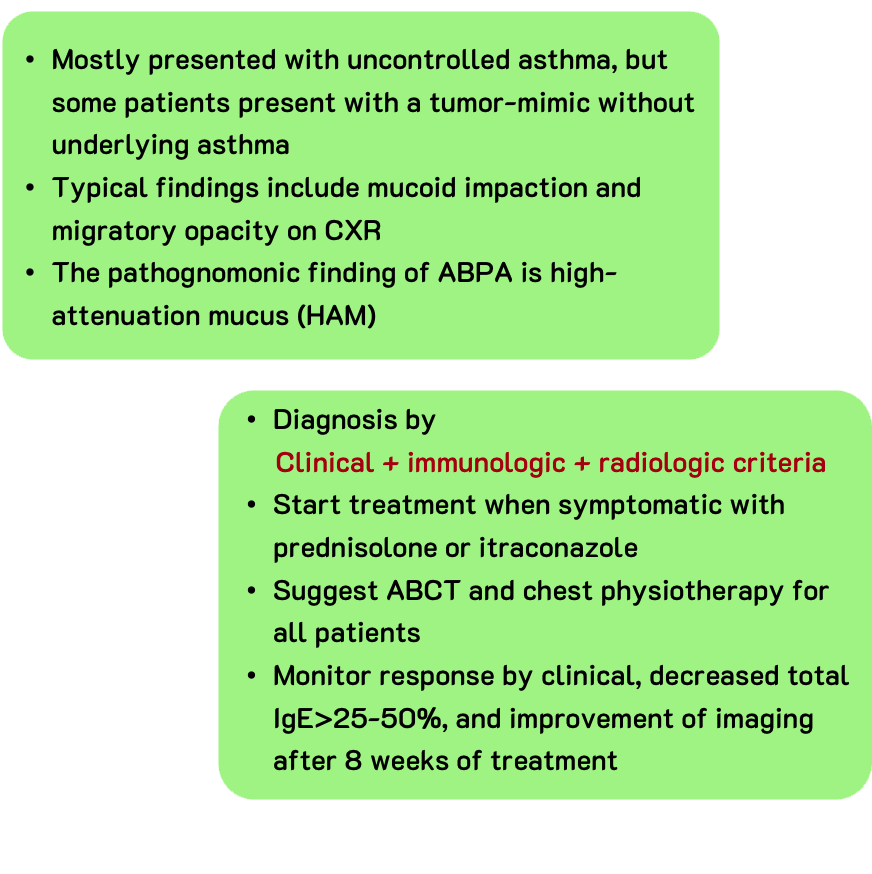
Diagnsosis
Allergic bronchopulmonary aspergillosis (ABPA)